Should You Open An ASC?
This is a question we deal with for every surgery client. The payment difference between facility owners and surgeons is significant. Although there are tradeoffs, we ultimately advise every surgical group to think over a 5–10 year horizon for how they might eventually own the place they do surgeries. The piece below shows how our clients have thought about the math. It makes estimates using the most recent Medicare prices for revenue, but when doing the math you should plug in your own numbers. If you want to dive deeper into how this question applies to you, book time with us and we’d love to talk through it.
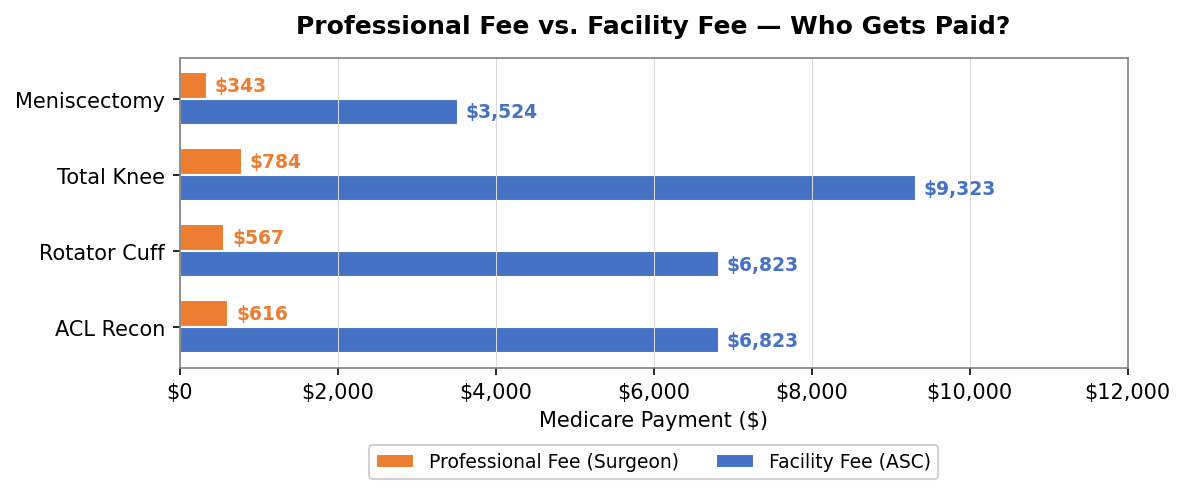
All billing questions in orthopedics start here: the surgeon gets 6 cents on the dollar.
We’ll use an ACL reconstruction as the example because it’s bread-and-butter sports medicine, but the pattern holds for basically every orthopedic surgery. When one of your patients tears their ACL and you take them through the full care journey (initial consult, MRI, surgery, post-op rehab), the total Medicare payment across all of those services is around $10,800.
Your professional fee for performing the surgery? $616.
The facility fee, which goes to whoever owns the room you operated in? $6,823.
The building gets paid 11x what you get paid. And this isn’t an edge case. Rotator cuff repair: $567 for you, $6,823 for the facility. Total knee: $784 for you, $9,323 for the facility. A knee scope that takes 30 minutes: $343 for you, $3,524 for the room.
CMS 2025 MPFS and ASC payment rates.
When you look at the entire care episode, nearly all the revenue is generated outside of the orthopedic clinic. Here is what the typical care journey will look like for an ACL patient at Medicare rates. I’ve bolded the parts that an orthopedic surgeon gets paid for.
- Pre-op revenue ($550): new patient consult / follow-up visit ($150 each), X-Ray and MRI imaging ($250 together)
- Surgery ($7.5K): professional fee ($616) and facility fee ($6.8K)
- Post-op revenue ($2.8K): follow-up imaging ($200), 24 physical therapy sessions ($2.3K), knee brace ($300)
Grand total: $10.8K (~$1K for surgeon)
You can see that broken out for different categories below.
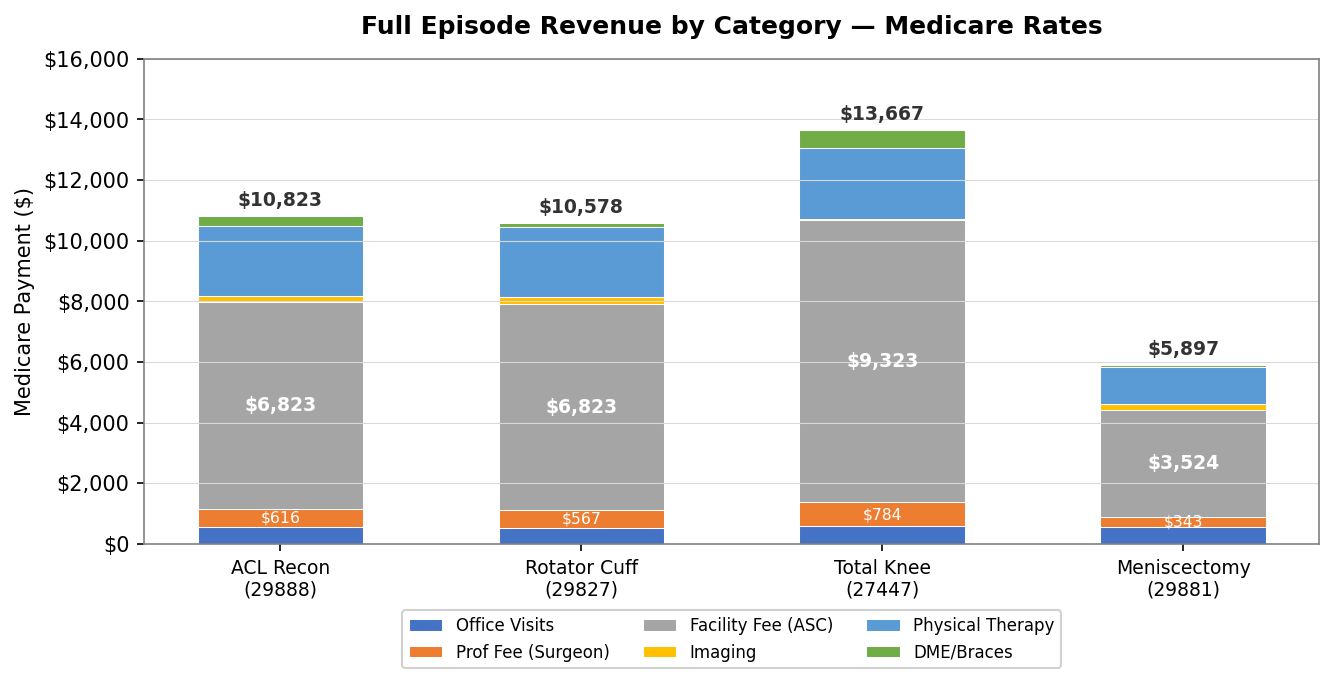
Full care episode revenue at 2025 Medicare rates, by category.
One key takeaway is how much money is captured in PT and imaging. We’ll cover the economics of in-office imaging and physician-owned PT in a separate post, as the topic deserves a bit more analysis.
OK, so… of course I’m buying the surgery center, right?
On paper, this is the compelling math which opens most of our client’s eyes towards the ASC opportunity. But the story is a bit more complex. The reason why Medicare pays such a high facility fee is that it expects high facility costs. That has a couple major categories:
- Rent: ASCs can cost $15–25K/month in rent if you’re looking at 5,000–6,000 feet of space
- Staff: ASCs require entire teams to run and operate smoothly. This includes suppliers for anesthesia
- Implants: This can be a heavy cost. Some commercial contracts will reimburse separately for implants, which blunts the impact. More on this in another post.
- Everything else: Malpractice insurance, equipment maintenance, utilities, IT, etc.
This can climb into the hundreds of thousands of dollars, in addition to what it costs to get in (between $2–6M in most conversations we’ve seen, although that can get much higher if the ASC is producing real money).
Of course, most of these costs are pretty much fixed whether you do 10 surgeries or 100. The real determinant of how successful your ASC will be is how many surgeries you can drive to it. The break-even point for most we look at is in the 125–200 range, but that may vary wildly depending on your contracts and scope of work.
That amount, however, is an achievable number for multi-surgeon groups, which is why we often end up advising these groups to explore their options. We don’t think every surgeon needs to buy an ASC tomorrow, but they’d be wise to start saving cash with an eye towards how to do it in the future. Every surgical group we work with that’s achieved real independence has done it by vertically integrating across one or more of imaging, PT, and ASC. After all, a surgeon collecting only professional fees captures about 6% of the value they create. A surgeon who owns the infrastructure captures north of 80%. That’s the difference between a job and a business.
Rates from CMS 2025 MPFS and ASC Payment Rates. Commercial estimates at 135% of Medicare. Operating costs from published industry benchmarks for 2-OR orthopedic ASCs. This isn’t financial or legal advice.